Blog
2 min read
The Weight Loss Candy, What You Need To Know
The "weight loss battle" is a common struggle for many, often involving a combination of dietary changes, exercise, and lifestyle adjustments to achieve a healthy weight.
O
Olah bute
August 17, 2025
907 views
ARTICLE BY SHINGIRAI SWISWA
09/05/24
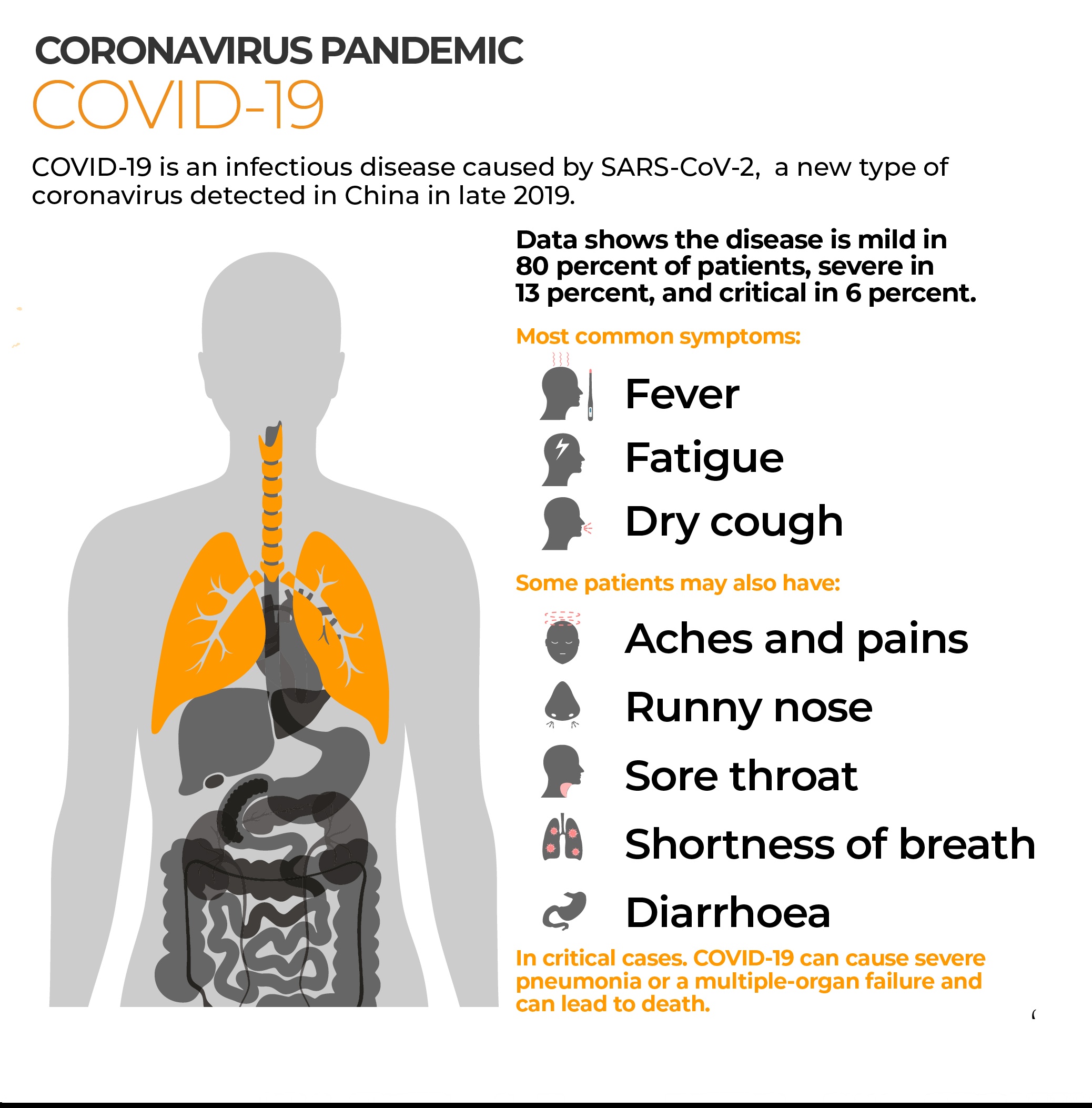
Zimbabwe and the rest of the world are fighting a war against obesity, which is fueling in part, the incidence and prevalence of Type 2 diabetes. Type 2 diabetes is a complex metabolic disorder characterized by hyperglycemia arising from a combination of insufficient insulin secretion together with resistance to insulin action. Studies have linked improved glycemic control with a reduction in the rates of diabetes-associated complications. Therein came our interest in incretin-based therapies namely
1)glucagon-like peptide-1 receptor (GLP-1R) agonists eg semaglutide (famous Ozempic),
2)glucose-dependent insulinogenic peptide GIP/ GLP-1R agonists eg tirzepatide (famous Mounjaro)
3) dipeptidyl peptidase-4 inhibitors (DPP-4i) eg sitagliptin (famous Januvia).
Both exert their actions through potentiation of incretin receptor signaling at the hormone level. For this purpose of this short article, we shall summarise issues regarding the efficacy and tolerability of medications with glucagon-like peptide-1 receptor (GLP-1R) agonists and glucose-dependent insulinogenic peptide receptor (GIP-R) agonists.
• After eating, circulating levels of GLP-1 and GIP increase rapidly and transiently.
• Take note that in the central nervous system (CNS), GLP-1 promotes satiety, which is synergistic with its effects on slowing gastric emptying and increasing gastric accommodation in promoting weight loss.
• Degradation-resistant GLP-1R or GIP/GLP-1 agonists have been developed since the hormones are prone to renal clearance and the DPP4 enzyme action.
• GLP-1 RAs and GIP/ GLP-1 RAs have gained popularity in treating obesity with or without diabetes. They appear to cause weight loss by slowing stomach emptying, stimulating centers in the brain that control appetite, and increasing the feeling of being full after a meal.
• Most commonly reported GI AEs with GLP-1 RAs oral or injectable versions are nausea, vomiting, diarrhea, and constipation. GIP/GLP-1 RAs are more tolerable.
• When a patient develops nausea, fullness, or vomiting during dose escalation, it may be prudent to slow down and keep the dose at a level that does not produce symptoms.
• Due to nausea, patients should be told not to continue eating after satiety.
References:
Drucker D et al 2010 (Diabetes Care)
Larkin M 2023 (Medscape)
09/05/24
Zimbabwe and the rest of the world are fighting a war against obesity, which is fueling in part, the incidence and prevalence of Type 2 diabetes. Type 2 diabetes is a complex metabolic disorder characterized by hyperglycemia arising from a combination of insufficient insulin secretion together with resistance to insulin action. Studies have linked improved glycemic control with a reduction in the rates of diabetes-associated complications. Therein came our interest in incretin-based therapies namely
1)glucagon-like peptide-1 receptor (GLP-1R) agonists eg semaglutide (famous Ozempic),
2)glucose-dependent insulinogenic peptide GIP/ GLP-1R agonists eg tirzepatide (famous Mounjaro)
3) dipeptidyl peptidase-4 inhibitors (DPP-4i) eg sitagliptin (famous Januvia).
Both exert their actions through potentiation of incretin receptor signaling at the hormone level. For this purpose of this short article, we shall summarise issues regarding the efficacy and tolerability of medications with glucagon-like peptide-1 receptor (GLP-1R) agonists and glucose-dependent insulinogenic peptide receptor (GIP-R) agonists.
• After eating, circulating levels of GLP-1 and GIP increase rapidly and transiently.
• Take note that in the central nervous system (CNS), GLP-1 promotes satiety, which is synergistic with its effects on slowing gastric emptying and increasing gastric accommodation in promoting weight loss.
• Degradation-resistant GLP-1R or GIP/GLP-1 agonists have been developed since the hormones are prone to renal clearance and the DPP4 enzyme action.
• GLP-1 RAs and GIP/ GLP-1 RAs have gained popularity in treating obesity with or without diabetes. They appear to cause weight loss by slowing stomach emptying, stimulating centers in the brain that control appetite, and increasing the feeling of being full after a meal.
• Most commonly reported GI AEs with GLP-1 RAs oral or injectable versions are nausea, vomiting, diarrhea, and constipation. GIP/GLP-1 RAs are more tolerable.
• When a patient develops nausea, fullness, or vomiting during dose escalation, it may be prudent to slow down and keep the dose at a level that does not produce symptoms.
• Due to nausea, patients should be told not to continue eating after satiety.
References:
Drucker D et al 2010 (Diabetes Care)
Larkin M 2023 (Medscape)